
Gradually, everything that was remotely protective for B12 deficient patients appears to be being deleted, eroded and changed to suit those who seem intent on switching us permanently to tablets which won’t help to repair nerves.
B12 supports the immune system, it is vital for life, injections are required to keep those of us who cannot absorb B12 from food well and functioning. The WHO list hydroxocobalamin as an essential medicine. Humans simply cannot live without it and should not be forced to, but that’s what’s happening now.
Those having injections regularly cannot absorb B12 from food, it is not dietary lack that brought them to their knees it was one of the other many causes of B12 deficiency.
Many are terrified to challenge their GP’s, many who have asked to be allowed to self inject have been ignored. Nurses are calling patients for their agreement to permanently switch their future treatment to tablets only. This must be resisted at all costs, see why below. Patients are already traumatised by COVID, separated from their loved ones and then have to deal without vital treatment because of a distinct lack of understanding of this very common and commonly misdiagnosed condition.
Things are changing day by day and there is no one sensible source of information for our GP’s. Some patients have had letters stating the GP’s are following advice from Public Health England, NHS England, CCG’s, etc and some even say ‘advice from Europe’.
The situation is an absolute disaster and needs sorting fast.
Patients need vital injections
Patients can be taught to give injections, we can be trusted, we are adults
Patients can then function, can do their Key work, can look after their families, can maintain mobility, can reduce pain levels and keep mental health problems at bay.
The BMA (British Medical Association) March
In March the BMA produced a traffic light workload prioritisation table for the RCGP.
Stating:
“………Past experience has shown that patients will die from non-COVID-19 related illnesses in addition to COVID-19 itself as we divert all of our health care resources towards it (1). General Practice has a huge role to play in maintaining the underlying health of our population in an attempt to prevent this. It is vital that we continue to provide care to all patients if we have the capacity, with workloads stratified to ensure that those at greatest need are prioritised.”
It uses the following headings:
GREEN – CONTINUE AMBER – IF POSSIBLE RED – STOP
B12 injections are under Amber as follows;
“Vitamin B12 injections – consider teaching appropriate patients to self-administer and ensure frequency is not more than 12 weekly”
(Not more than 12 weekly eh? That’s not what NICE say – see below!).
BMA April
B12 injections have since been downgraded by the BMA and the headings have been changed, only a few are now considered “Medium Priority” as of April the 10th 2020.
Amber – Medium Priority
“Vitamin B12 injections for post bariatric surgery patients – consider teaching appropriate patients to self-administer and ensure frequency is not more than 12 weekly. Review whether oral supplementation would be appropriate”.
Red – Lower Priority
“Vitamin B12 injections – consider teaching appropriate patients to self-administer and ensure frequency is not more than 12 weekly. Review whether oral supplementation would be appropriate if asymptomatic with a dietary deficiency ” BMJ 2019 https://www.bmj.com/content/365/bmj.l1865
The question is, why during this crisis, isn’t our immunity boosting, life saving vitamin injection for people who can’t absorb B12 from food in the Green band? It simply doesn’t make any sense.
This is what NICE CKS states, that if B12 deficiency is;
• Not thought to be diet related — administer hydroxocobalamin 1 mg intramuscularly every 2–3 months for life.
• Thought to be diet related — advise people either to take oral cyanocobalamin tablets 50–150 micrograms daily between meals, or have a twice-yearly hydroxocobalamin 1 mg injection.
British Society for Haematology (BSH) is moving goal posts;
BSH advice during the COVID19 pandemic now decide that those of us who rely on B12 injections can now access our non existent liver stores, here’s an excerpt below;
Liver stores last for a year and hence levels of B12 will not be affected if one to two 3 monthly injection is omitted in patients on maintenance parenteral B12 supplements. BSH supports omitting B12 injections even in this group during COVID19 outbreak at least until the surge has passed.
For patients who report symptoms in the weeks preceding B12 injection, oral B12 50-150 micrograms per day can be offered as an alternative because there will still be sufficient absorption. If still very symptomatic then B12 injection can be given with clear understanding that the interaction with healthcare increases transmission risk of COVID19. We suggest taking the opportunity to measure B12.
FAO/WHO 2001. Human Vitamin and Mineral Requirements. Chapter 5.
“…..Interruption of this so-called enterohepatic circulation of vitamin B12 causes the body to go into a significant negative balance for the vitamin. Although the body typically has sufficient vitamin B12 stores to last 3-5 years, once PA has been established the lack of absorption of new vitamin B12 is compounded by the loss of the vitamin because of negative balance. When the stores have been depleted, the final stages of deficiency are often quite rapid, resulting in death in a period of months if left untreated.”
Oral B12 research
Patients during the crisis are now regularly told that they can in fact absorb B12 from cyanocobalamin tablets and yet:
A review from Cochrane; (Wang et al., 2018) details this: ……
No study reported on clinical signs and symptoms of vitamin B12 deficiency (e.g. fatigue, depression, neurological complications), health-related quality of life, or acceptability of the treatment scheme.”
Authors’ conclusions: “Low quality evidence shows oral and IM vitamin B12 having similar effects in terms of normalising serum vitamin B12 levels, but oral treatment costs less. We found very low-quality evidence that oral vitamin B12 appears as safe as IM vitamin B12. Further trials should conduct better randomisation and blinding procedures, recruit more participants, and provide adequate reporting. Future trials should also measure important outcomes such as the clinical signs and symptoms of vitamin B12 deficiency, health related-quality of life, socioeconomic effects, and report adverse events adequately, preferably in a primary care setting.”
The Difficulties With Vitamin B12
https://pubmed.ncbi.nlm.nih.gov/27009308/?i=5&from=b12
A 22-year-old woman presented with progressive sensory ataxia and optic neuropathy. Previous investigation by her general practitioner had found a low serum vitamin B12, which had been corrected with oral supplementation. Neurological investigations showed raised plasma homocysteine and methylmalonic acid towards the upper limit of normal with a low serum vitamin B12 MRI showed an extensive cord lesion in keeping with subacute combined degeneration of the spinal cord. We treated her with high dose parenteral vitamin B12 and she has made a partial recovery. We discuss the management of patients who present with neurological manifestations of vitamin B12 deficiency; highlighting the fact that parenteral replacement is needed in such cases, even if the serum vitamin B12 level appears to be normal. We also discuss ancillary investigations that should be performed in patients with suspected vitamin B12 deficiency.
Caution note from the B12 institute about oral supplements .
____________________________________
Everyone making the rules is watching the smoke but not one is seeing the fire…..
People in crisis sometimes make bad decisions and stopping B12 injections is one of them, it’s short sighted and harmful and there will be a price to pay if things don’t change soon.
A simple solution would be to allow us to buy injectable B12 OTC as is allowed in many other countries, which leads me to my next blog.
Best wishes and keep safe
Tracey
(Thank you Dr Katie Brooks for finding WHO ref)
I cannot be without my injection, would happily learn to do it myself, suggested it once to gp and she said organising all the sharps and sharp collection would be as expensive as me popping into the surgery to have it. I have it 6 weekly and barely manage on that, the week and a half before the injection is hell in my house, I drop everything, cannot concentrate, everything hurts and my other complaints get worse. I cannot sleep, I have dry mouth and burning mouth syndrome in that time which clears up about a week after injection. Please don’t let them take this life saving injection away. My father and all his sisters suffered from pernicious anaemia and towards my dads end, he was 83, he was having his injection weekly.
The “guidance” on liver stores from the BSH is seriously misinformed. B12 from the liver is released into the small intestine via the bile. Absorbing it from there relies on exactly the uptake mechanisms that don’t work in people with pernicious anaemia or other absorption issues.
“In addition to causing malabsorption of dietary vitamin B12, PA also results in an inability to reabsorb the vitamin B12 which is secreted in the bile.”
Reference: FAO/WHO 2001. Human Vitamin and Mineral Requirements. Chapter 5.
http://www.fao.org/3/y2809e/y2809e0b.htm?fbclid=IwAR2rCHBGSZAIxliwUEIcTp9P-OgHg-19_RFyv96pU0c6G9MJ61FG8RjCu_8
B12 for some people is their life source like insulin for T1 diabetics. Why not allow a person to self inject like with insulin? Its negligence by Public Health England!
The BSH “guidance” about liver stores is extremely misleading. B12 from the liver is released into the bile and ends up in the small intestine just as it does from food. So people with pernicious anaemia or other absorption issues can’t make use of it.
“In addition to causing malabsorption of dietary vitamin B12, PA also results in an inability to reabsorb the vitamin B12 which is secreted in the bile.”
Reference: FAO/WHO 2002. Human Vitamin and Mineral Requirements. Chapter 5: Vitamin B12. Available from: http://www.fao.org/3/y2809e/y2809e0b.htm
Thank you Katie, I will add this link to the blog and credit you. Best wishes Tracey
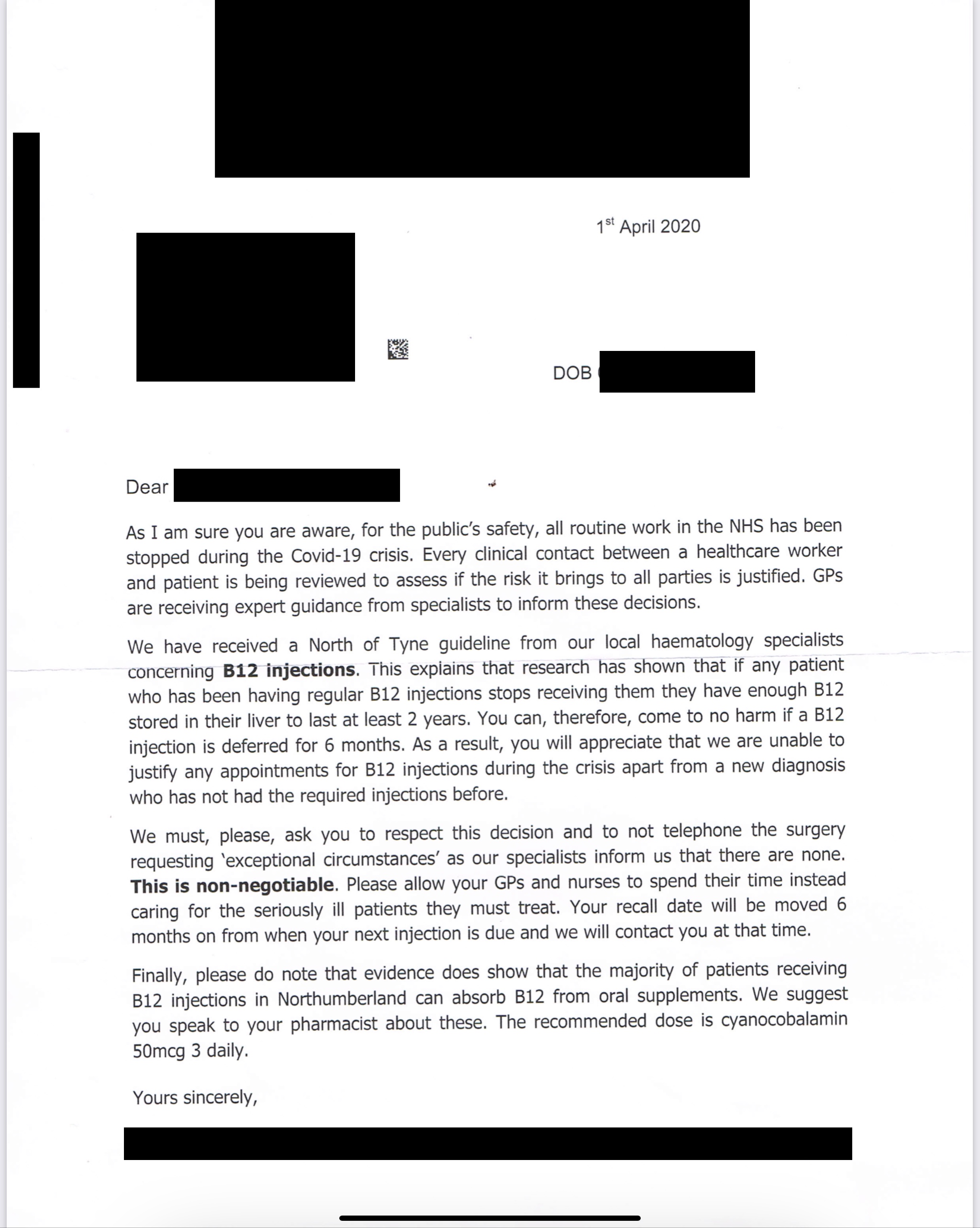
I can’t believe some of the letters doctors are sending to patients at the moment. Every day logging into support groups wondering what on earth I’m going to see next. Unreferenced comments about mysterious “new guidelines”, or vague references to “new research” (unspecified). GPs spending seemingly idle hours rifling back in time through patient records to see if they can remove injections altogether, COVID or not. Then telling people the good news, congratulations! It looks like you don’t need to have these pesky injections after all! Must have been a mistake to have you on them all these years… Stores that last 1 year, or is it 2 or 3? Depends whose writing. Patients with malabsorption being given dietary advice on sources of B12 in food. Patients proactively asking to self inject being told categorically no, for no good reason. Some being told too much B12 is dangerous or addictive (there’s no UTL so utter nonsense). Often the inexplicable contradiction that the injection is dangerous in excess and/or addictive, but we’ll give you tablets they’re OK. It’s all B12 so how can one be a problem and the other not? One of my personal favourites – we won’t give you your B12 injection but you can have a blood test instead – surely just as much close contact if not more needed for that one. It just goes on and on. But despite all that, just WOW to the letter you’ve posted in this blog. Non-negotiable. Don’t bother calling us because we don’t care one iota about how you feel, how sick you might be, clinical picture? Pft. It’s beyond heartless. There is just one common theme in all of this: we want you off injections and if possible we want you off them for good. We might be suggesting useless tablets instead, or in many cases we might just stop your treatment altogether. It’s a national scandal. We have Chris Whitty and Sir Patrick Vallance on the TV almost daily urging people to still use the NHS, it’s still open for business for non-COVID issues. They clearly haven’t spent any time down in general practice. Some of them, not all I grant you, but definitely a significant number, are most definitely not open for business for B12d sufferers.
This is seriously scary Nhs playing God! It’s not like the injections are expensive to buy -Europe they can be bought over counter .
Same is happens with T3 patients
Plugged pulled with many ! Why
I’ve seen a copy of this particular GP letter before, and I really think it merits a formal complaint. No decision that stops essential treatment for a diagnosed lifelong condition should ever be described by doctor to patient as “non-negotiable”. As I understand it, patient consent is still required.
I’ve long regarded GPs as essentially rogue in the way they interpret guidelines and evidence for diagnosis and treatment. They have also been given far too much power as gatekeepers for the NHS.
Thank goodness I know how to treat myself for PA, but many do not, or cannot afford to do so.
I need B12 injections every two weeks, a blood test results was missed by my Doctors, and for ten years I thought I was dying,Doctors eventually found results and given six doses over two weeks, and then onto twelve weekly, we found after two weeks symptoms returned, so I was sent to see Haematologist who was happy for me to have a dose every two weeks, this went on for years, I was fine got on with life no problems, until my regular nurse left, then a know it all nurse went over the head of my Doctor, and I was put on every twelve weeks, I now send for injections from abroad, but cannot give them my self, but my lovely husband taught himself to give my injection so I have one at twelve weeks at my Doctors, and the rest at home, but now have a letter saying they are not giving it at all, why do people who have no idea what it feels like to be short of B12 make these stupid decisions
When you look at COVID19 patients, 3 of the main treatments for those in ICU are vitamin D, vitamin C and vitamin B12…….
I am presently taking a sub lingual vitamin b12.
My GP said my level was sufficient but for at least 4 years I felt dreadful.
I as then tested for celiac but this was negative.
My symptoms continued, dull headache, palpitations, lack of concentration, raw tongue, tingling palms of hands and soles of feet, fatigue, depression.
It was an effort to keep working. I asked for shorter shifts and lighter duties for a time.
Eventually I took a years sabbatical and went abroad to try nurse myself better.
It was there I sourced the sub lingual vitamin b12 and within days my headache lifted, my palpitations stopped.
It took longer for the tingling in hands and feet to subside and my tongue to feel better.
I can honestly say I was amazed.
I cried as I had suffered for years with no help and all the time something so simple was available but never was it suggested as my levels were “acceptable”
Can sub lingual method be a substitute for injections during this Covid 19 pandemic?
Dear Hazel, thank you for your comment.Our GP’s have been done a great disservice by not being taught enough about B12 – or nutrition as a whole. It’s great to hear sublingual works for you, sadly they don’t help everyone.
Best wishes Tracey
Can i ask what product you use ?
Here is another reason not to stop B12… it is key to methylation and this study showed that cytokine storm more likely in people with poor methylation of genes-
Epigenetics of Delirium and Aging: Potential Role of DNA Methylation Change on Cytokine Genes in Glia and Blood Along With Aging https://www.frontiersin.org/articles/10.3389/fnagi.2018.00311/full
PS still giving b12 where I work
Thank you David!
When people can get any other vitamin over the counter, why has B12 injections been singled out as cannot buy over the counter?
Our health is at risk by being denied our injections.
Im quite lucky,ive got mine last month at my Doctors surgery,nurse came out shouted me in and got it